ABMI
Main menu:
- Home
- About ABMI
- Clinical Focus
- Monitoring Software
- TCD Systems
- Clinical Studies
- News/Investors
- Contact Us
The Embol-ADD PWD for real-time emboli monitoring in the OR
Monitoring Software > Real-Time Emboli Classification Software: Embol-ADD PWD
INTRODUCTION
Cerebral complications - stroke and neuropsychological disorders - after both cardiac and carotid surgery are now recognized as a serious and costly healthcare problem, mandating immediate attention for the estimated 1.5 million patients undergoing such surgery through the world annually.
Neurological complications in CABG
The incidence of neurological complications after cardiac and carotid surgery depends on the type of surgery, and on the neurological and neuropsychological parameters taken into consideration. For example, in coronary artery bypass graft (CABG) surgery, 3 % of patients undergo a massive stroke or a post-anoxic encephalopathy. If one looks also at more subtle neurological complications including cognitive decline, the rate climbs to 33 % - 75 % depending on studies
Based on the results of 24 US medical centers, 6% of patients suffer adverse cerebral events after CABG, including death, stroke, or substantial deterioration of intellectual function. In some subgroups of operated patients, the rate of neurological complications can even increase : 1 in 6 patients will develop cerebral complications that are frequently devastating and costly after a valve replacement combined with coronary revascularization.
Overall incidence of neurological complications in cardiac surgery
The overall incidence of cognitive decline after cardiac surgery is variable, ranging from 40-50 % of patients to 79 % in the early postoperative period, whereas the incidence of cognitive disorders at 6 months ranges from 19 % to 57 % [all references available].
One way to estimate the socioeconomic impact of neurological complications of cardiac surgery consists in evaluating the capability of patients to reintegrate their socioprofessional activities. For instance, 25 % of patients abandon their professional activity for neurological reasons 5 years after a valvular replacement surgery.
Carotid endarterectomy and stroke
Carotid endarterectomy (CE) which is performed approximately in 400,000 patients through the world yearly, is also associated with a combined mortality and morbidity rate of 5 % to 11 %. The 30-day mortality rate linked to CE is 1-2 % and is explained by myocardial infarction, stroke, brain hemorrhage, cranial nerve injury and hemorrhage at the surgical site. The reported perioperative stroke rate associated with CE ranges from 5 % to 8 %]. Moreover, MRI brain studies revealed 5-10 mm diameter subcortical infarcts occurring after CE in approximately 10 % of patients.
Emboli cause stroke, neurological decline and neuropsychological deficit
Neurological decline and in particular stroke which represents the first cause of permanent physical/intellectual disability in Western countries - and neuropsychological deficits resulting from cardiac surgery as well as carotid surgery are most likely attributed to brain embolism of air or particulate matter. Brain macroemboli (> 200 µm in diameter) - associated with atherosclerotic plaque disruption - are believed to provoke focal neurological deficits such as stroke, whereas particulate microemboli (< 40 µm in diameter) - consisting of white cells and platelet aggregates, fat or air - may be implicated in more subtle diffuse cerebral dysfunction such as cognitive disorders.
Solid versus Gaseous emboli
Gaseous emboli are believed to be infrequently associated with cerebral ischemia, whereas solid or particulate microemboli are considered responsible of neurological / neuropsychological complications of both cardiac and carotid surgery. Transcranial Doppler (TCD) is to date the sole technique that permits the monitoring of perioperative brain embolism (macro- or microembolism) in real time.
Improving the neurological outcome through real-time monitoring of solid and gaseous embolization with TCD
Because neurological as well as neuropsychological disorders represent a crucial medical and socioeconomic problem in cardiac and carotid surgery, new neuroprotection strategies are required in the OR. Studies have shown that immediate feedback information from TCD monitoring - hemodynamic and embolic information - can prompt the vascular surgeon to modify the planned course of surgery thereby reducing neurological and neuropsychological complications.
Also, real-time monitoring of solid embolization in the OR (where no clinical neurological examination is possible, e.g. for anesthesized patients) can prompt the surgeon to administer recanalyzing or neuroprotective drugs as needed, and this can be done right upon stroke onset. Indeed, waiting until the patient is sufficiently awake in the post-op period to perform a neurological exam means wasting critical time. As stroke fighting medication have an effectiveness window of typically 3-6 hours after stroke onset, wasting such critical time means wasting the patients brain.
ABMIs SOFTWARE OFFER FOR THE OR MONITORING MARKET
ABMI takes its origins in an academic research project which was conducted jointly at the Geneva and Lausanne University Hospitals in Switzerland, in collaboration with the Swiss Federal Institute of Technology and the Universities of Lausanne and Geneva. The aim of our interdisciplinary team of neurologists, surgeons and engineers was to develop a system that could detect emboli in real time in the middle cerebral artery through TCD, and that would be able to efficiently separate solid form gaseous events.
At first, ABMI has developed an off-line application the Embol-STATION ® - which can analyze TCD data files after patient monitoring. The Embol-STATION has been the subject of various clinical studies and its classification rates are 96% for emboli versus artifacts, and 92% for solid versus gas, based on some 4000 events.
Recently, the algorithms of the Embol-STATION have been adapted to the constraints of real-time without compromising on classification power. Therefore, we are able to propose today a software add-on module that will integrate easily with your current TCD software and that will perform emboli detection and solid-gas separation in real-time: this is the Embol-ADD.
ABMIs Embol-ADD can be customized to your needs:
- The Embol-ADD can be limited to emboli detection, for instance, and that application could be installed on all your TCD systems, while the solid/gas separation features would be available as an option,
- The Embol-ADD can be easily combined with the off-line analysis software Embol-STATION for immediate and more in-depth re-analysis of the TCD signals recorded during a procedure, and for the documented reporting of those,
- The Embol-ADD easily integrates with your existing TCD software and runs on any type of operating system. We propose two options for such an integration:
- The LIMITED integration option: your TCD software transfers the raw Doppler signals
to the Embol-ADD, which analyses it and displays the results in a window which is independent
of your TCD software,
- The FULL integration option: the Embol-ADD is a hidden computation engine which receives
the raw Doppler form your TCD software and sends back to it the embolization data in the form
you like. Such embolization data can then be displayed by a display in your TCD software.
More details on this are given below.
Future evolutions of the Embol-STATION and the Embol-ADD will include, e.g., the estimation of the sizes of solid emboli, as these sizes are not correlated with the signal intensity in dB and therefore needs finer algorithmic tools to be determined.
PRODUCTS DETAILS: ABMIs EMBOL-ADD®
The Embol-ADD® detects, counts and identifies brain emboli (as solid or gaseous) in real time.
Based on the Embol-STATION, of which it shares the algorithmics, the Embol-ADD is the obvious software evolution optimized for real-time functioning. The Embol-ADD PWD is optimized for Pulsed Wave Doppler (PWD) systems and is currently being adapted onto transcranial Doppler systems manufactured by worldwide leaders in the field.
The Embol-ADD PWD screen is simplified with respect to that of the Embol-STATION, and is limited to showing the essential information. As OEM software, it will be integrated in the TCD manufacturer's display.
The Embol-ADD is available on a OEM basis. TCD producers, please contact us!
SOFTWARE INTEGRATION
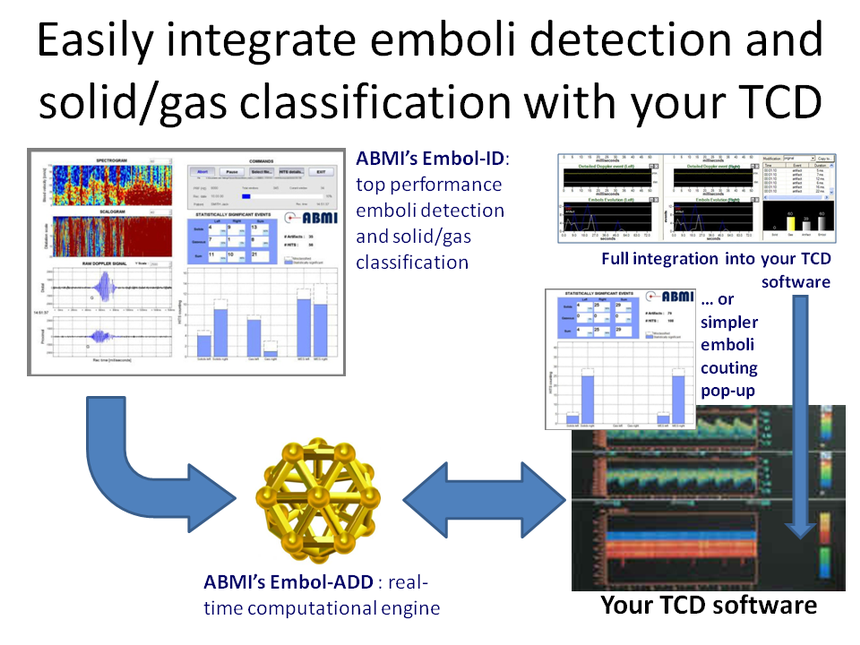
Regarding the integration of our software with your TCD system and software, we have two options (illustrated above):
1. LIMITED INTEGRATION OPTION: our software will be a pop-up window and will run in parallel to yours.
- We shall provide you with our specs for the real-time data transfer from your TCD application to our emboli detection and classification solution.
- The signal will be analyzed by our software and the results about embolization will be displayed in real time in a window which is independent from your TCD software.
- The presently available display windows are shown in the pictures below. The displays show the solid/gas evolution in time, the total counting for solids, gas and artefacts, the HITS intensity versus time, etc.
- We can also design the pop-up window according to your needs, depending on what you would like to be displayed (emboli counting, solid/gas counting, side (L/R), histograms, time evolution of embolization, etc).
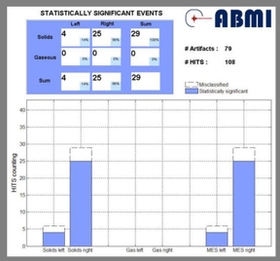
Example 1: real-time window showing the total counts for solids and gas on the left and right sides, plus the horizontal and vertical sums (total right, total left, total solid, total gas) as well as a histogram for solid, gas and artifacts.

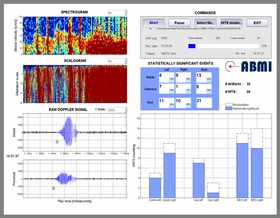
Example 2: real-time window showing a listing of high-intensity events (HITS), a display of the evolution in time of the solid and gaseous embolization, and the distribution of the intensities of the events. Various oparameters can be adjusted and data files can be reread.
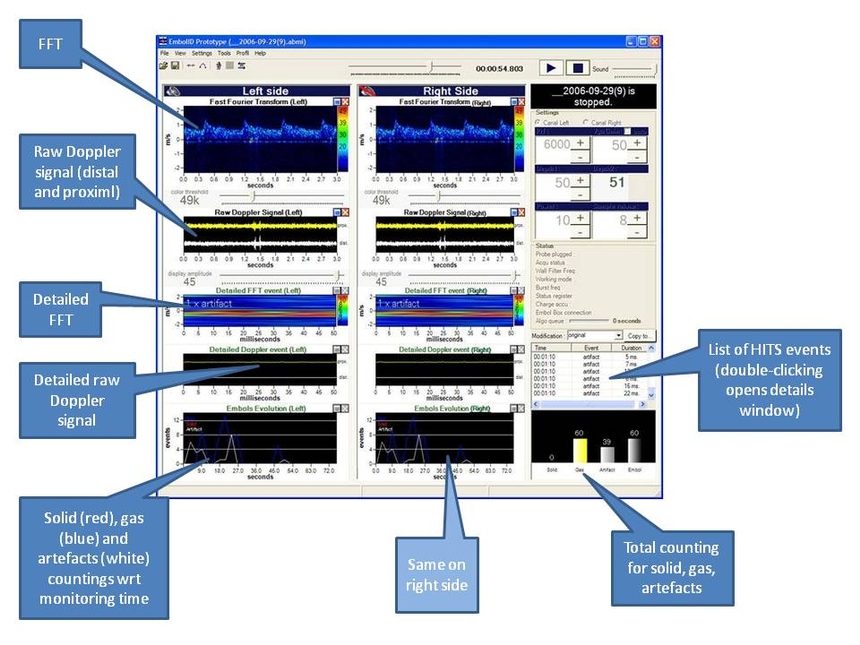
Example 3: all the elements of the Embol-STATION display can be considered for designing your own interface. In any case, the Embol-STATION can be included in your package for the off-line detailed re-analysis of data files acuired with the Embol-ADD during procedures.
2. FULL INTEGRATION OPTION: our application is an invisible computation engine which works in the bakground and you design your own window for displaying results.
We provide you with the in/out specs (the raw Doppler signal goes in, the emboli countings come out)
you use the data provided by our application (solid/gas emboli countings) to animate a display that you will design in your own TCD software.
Please note that we have code which does this and displays embolization, and we could provide that code together with the emboli classification engine. The interface (shown below) is still a prototype but the display elements can be extracted and provided to you.
COMPATIBILITY ISSUES
There will be NO problems at the level of software compatibility, since our software is widely compatible with PC, Unix, Linux, etc.
Sub-Menu:
- The Embol-ADD PWD for real-time emboli monitoring in the OR ←
- Embedded Technologies
- Applications, Features and Benefits